
What is “Carpal Tunnel Syndrome”
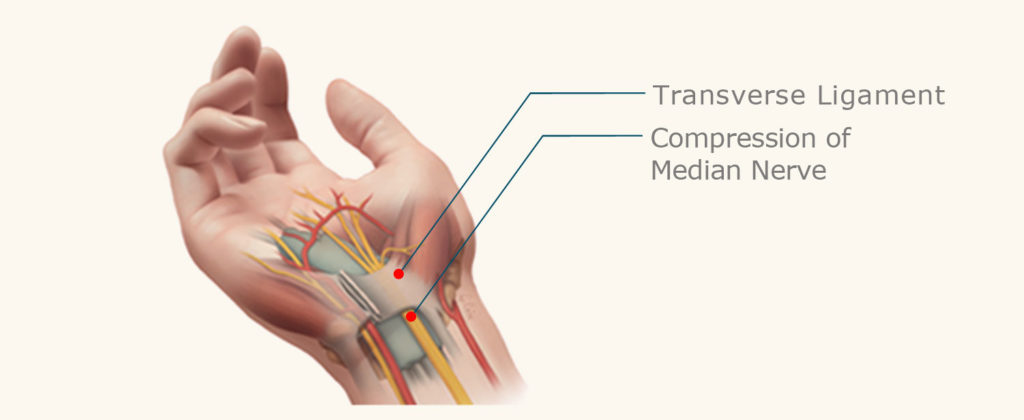
We all normally have a carpal tunnel but we do not necessarily have “Carpal Tunnel Syndrome”. The Carpal Tunnel is an arch formed by the wrist bones and the carpal ligament on top. This anatomical structure resembles a tunnel with a road + the hole in the mountain.
The Carpal tunnel is normally very crowded. Many structures traverse it on their way from the forearm to the hand. Nine tendons from the forearm muscles (two per finger except the thumb) traverse the tunnel to flex the digits. But the most sensitive and the most delicate structure traversing it is the MEDIAN NERVE. In some predisposed people, the tunnel is rather narrow and any slight swelling of the tendons (tendinitis) inside this unyielding structure can increase the pressure and compress the median nerve. This typically occurs at night when we normally accumulate fluid or after extensive use of the hand when the tendons swell.
When the nerve is compressed, the patient feels pain, tingling, pins & needles, numbness, clumsiness, weakness. With time, the nerve ceases to function well and the fingers become numb, the hand weak and more clumsy. Typically patients will complain that they are dropping objects from their hand or that they have trouble buttoning their clothes. When we find evidence that the nerve is not functioning normally, we recommend release of the carpal tunnel to relieve the symptoms, prevent more permanent damage and muscle loss.
Carpal Tunnel Symptoms
The main symptom of carpal tunnel is tingling in the fingers (except for the little finger). The sensation is often similar to the tingling sensation experienced when your feet fall asleep. People suffering from carpal tunnel have worse symptoms at night and often wake up with the need to shake up their hand at night. As the carpal tunnel problem worsens, the pain becomes more constant and the hands become weaker and clumsier. As the disease progresses, the fingertips become more numb and hand function deteriorates. The median nerve innervates the muscle that causes the thumb to oppose to the other fingers. Weakness and then atrophy of this muscle which is irreversible significantly impairs hand function. Unfortunately, because the problems develop slowly over time, many patients accommodate to the problem and present with very advanced disease when the nerve is dead and the muscles are gone.
Causes Of Carpal Tunnel
There are many causes for carpal tunnel syndrome. Most importantly is a probable genetic predisposition. Some people’s tunnel is just narrower than others and in some people the tendons tend to swell more than others after the same amount of activity. Other conditions associated with carpal tunnel syndrome include:
- Diabetes. Nerve compression is poorly tolerated in diabetics who are also predisposed to diabetic neuropathy.
- Thyroid diseases (typically hypothyroidism)
- Obesity (Fat in the tunnel can also compress the nerve)
- Pregnancy
- Menopause and hormonal therapy
- Rheumatoid Arthritis
- Wrist & Hand Injuries
Contrary to popular belief, typing on the keyboard is not really a cause of carpal tunnel syndrome. If it were, we would have a catastrophic epidemic public health issue since millions of people spend their time on the keyboard. It is only after prolonged, un-usual, extensive overuse of the hands that carpal tunnel could emerge; and this only in predisposed individuals.
Treatment of Carpal Tunnel
Splints
If your symptoms are minor, splinting may help. Full flexion and extension of the wrist makes the carpal tunnel narrower. A splint forces the wrist to remain straight in the position where the tunnel is widest and this lowers the compression on the nerve. The splint should be worn at night or during manual activities that may cause the tendons to swell. When symptoms and problems persist despite the splint, surgical release of the tight carpal tunnel is indicated to prevent further irreversible nerve and muscle damage.
Cortisone Injection
If the carpal tunnel problem continues despite the wrist brace, the next step might be a cortisone injection. Cortisone is a steroid that is used to treat inflammation. While it may make the patient feel better temporarily (for a few weeks or months), it does not treat the underlying carpal tunnel problem. The injection of cortisone is a controversial issue. With cortisone injection, the nerve and muscle damage will continue to worsen silently without the patient realizing he is getting worse. While doctors sometimes recommend an injection, repeated injections may cause complications with the patient’s tendons and will impair the recovery after the eventually required surgical release.
Carpal Tunnel Surgery
Surgery for carpal tunnel release involves cutting the carpal ligament, this is the tough, inelastic structure that forms the roof of the tunnel. Cutting the entire ligament enlarges space, releases the pressure in the carpal tunnel and frees up the median nerve in order for it to recover. There are two ways to achieve the release: The old open release and the more advanced endoscopic technique.
Open Carpal Tunnel Release Surgery
The open release is an old operation, still performed by surgeons who are not experienced enough, or are not comfortable enough, with the modern minimally invasive endoscopic procedure. The open carpal tunnel release requires cutting the skin in the palm lf the hand and then performing an extensive dissection deep in the middle of the palm. Because of the inherent long recovery and delay in the return of hand function with this invasive surgery, the open carpal tunnel release was considered a major operation till the advent of the endoscopic technique.
Endoscopic (Minimally Invasive) Release: The Advanced technique
The endoscopic technique requires a tiny, less than 1 cm incision in the forearm, just above the wrist. Through this tiny hole, we insert a camera and the operation is performed with the use of a large TV monitor. The camera has on its tip a tiny laser sharp blade that can simply slice the ligament without bothering any of the surrounding structures. The procedure takes less than 5 minutes, is often done under local anesthesia (with some minor sedation if needed), and leaves no scar. The patients are allowed to return to gentle use of their hand immediately after the procedure. But are warned not to use force for a month or so till the divided ligament heals in the more open position.

What to Expect After Surgery
There are no sutures to remove, the tiny incision is simply closed with a fine stich that dissolves on its own over the first 10 days. The patient can use their hand immediately after surgery for gentle activities and are instructed to refrain from using the operated hand for anything that requires force for about one more month till the ligament heals in the more open position. Immediately after surgery the night pain and the tingling should disappear. Patients typically say that they are able to sleep well for the first time. But it may take longer before pain and numbness disappear completely. This is because the crushed nerve has to slowly recover before things return to normal. If the operated hand is your non-dominant hand you may return to work within 1 – 2 days after surgery but most patients wait longer. If the operated hand is your dominant hand and work requires repetitive tasks it is strongly recommended to wait 6 – 12 weeks before returning your hand to normal tasks.
